Quick Facts
- Average Onset: Mid-40s, though it can begin as early as age 30.
- Duration: Typically 4 to 10 years, ending one year after the final period.
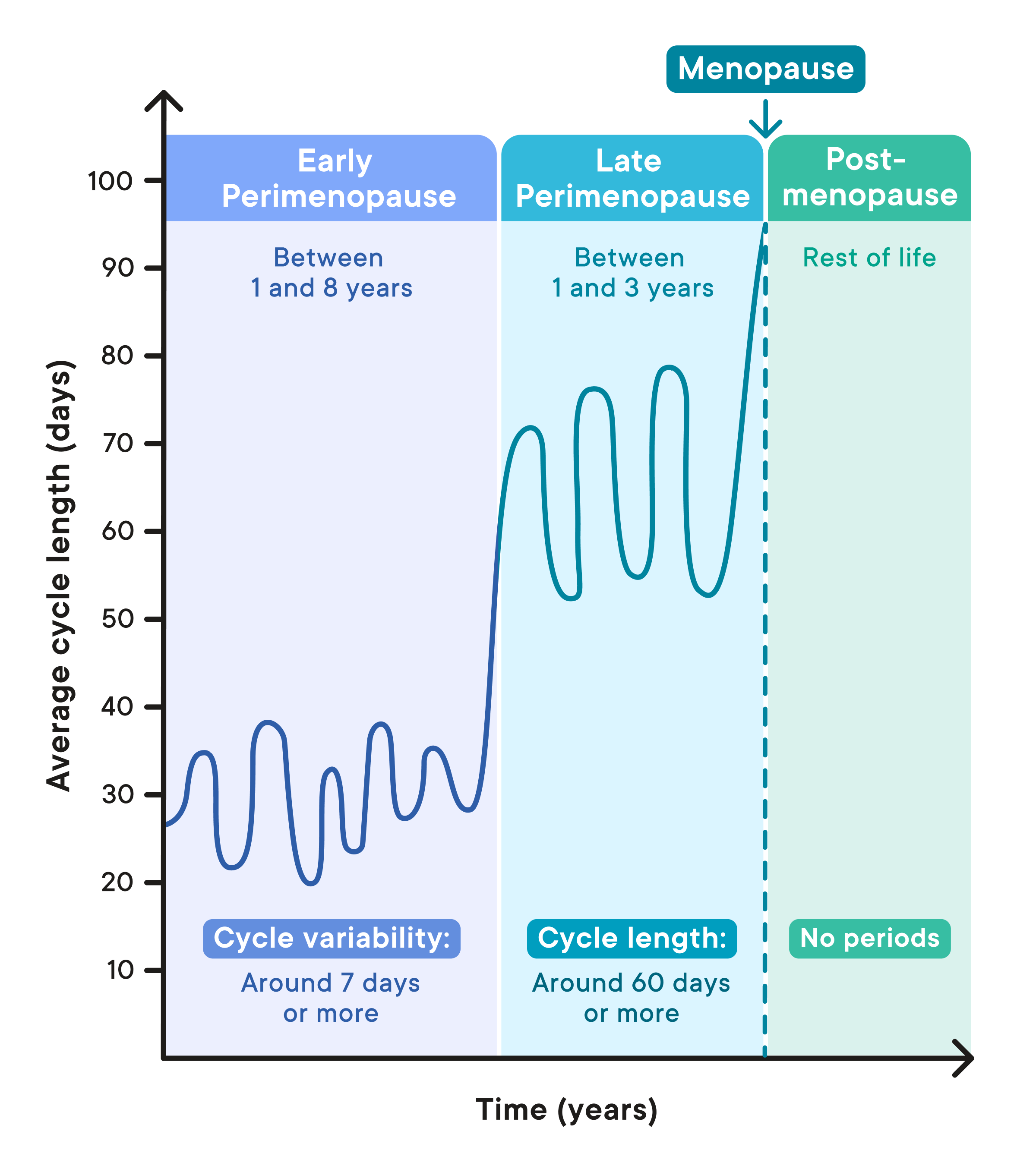
- Early Marker: Menstrual cycle length variability of 7 or more days (e.g., a 21-day cycle followed by a 29-day cycle).
- Primary Cause: Recalibration of the hypothalamic-pituitary-ovarian axis and erratic ovarian function.
- Cognitive Impact: Up to a 25% temporary drop in brain glucose metabolism, often causing brain fog.
- Clinical Recommendation: Focus on longitudinal symptom tracking and metabolic health through resistance training and Vitamin K2.
Perimenopause is a complex neuroendocrine transition, often beginning in the early 40s. Understanding perimenopause symptoms and the hypothalamic-pituitary-ovarian axis is key to managing this change. It is a period of high hormonal volatility where the body recalibrates, leading to shortened menstrual cycles, hot flashes, and cognitive shifts.
The Early Indicators: Recognizing Your First Shifts
For many women, the first hint that something is changing isn't a hot flash, but a subtle shift in the calendar. Clinical frameworks like the STRAW+10 (Stages of Reproductive Aging Workshop) classify this as Stage -2. During this phase, the communication between your brain and your ovaries begins to lose its crispness. Your brain releases more follicle-stimulating hormone to nudge the ovaries into action, but the response is often unpredictable.
One of the most reliable early signs of perimenopause is a change in your cycle length. You might notice your usual 28-day cycle suddenly shrinking to 24 or 21 days. This happens because the follicular phase—the time it takes for an egg to prepare for release—shortens. While many associate the transition with the mid-40s, research indicates that more than 55% of women aged 30 to 35 report experiencing moderate to severe symptoms associated with the transition.
Identifying early signs requires looking beyond just the pelvic region. Early perimenopause symptoms frequently include the sudden onset of night sweats or a feeling of being "wired but tired" before bed. These are not just physical annoyances; they are signals from your nervous system that your internal thermostat is reacting to the first ripples of estrogen volatility. Managing irregular periods during perimenopause transition starts with recognizing that these fluctuations are a physiological recalibration rather than a breakdown of the system.
Inside the Chaos Phase: Why Hormones Go Wild
There is a common misconception that perimenopause is a slow, steady decline into low estrogen. In reality, the early years are often a "Chaos Phase" characterized by dramatic spikes. During this time, estrogen levels do not simply decline but often fluctuate chaotically, sometimes averaging 30% higher than during a woman's peak reproductive years.
This surge occurs because the endocrine system is working overtime. The hypothalamic-pituitary-ovarian axis is trying to maintain ovulation, leading to "luteal out-of-sync" events where you might have two peaks of estrogen in a single month but very little progesterone to balance it out. This progesterone deficiency is often the culprit behind the heavy periods, breast tenderness, and increased irritability that many women experience during their late 30s and early 40s.
Because of this extreme estrogen volatility, a single blood test is rarely helpful. Serum hormone panels taken on a Tuesday might show perfectly "normal" levels, while by Thursday, those levels have tripled or plummeted. This is why clinical diagnosis focuses on your reported history and symptom patterns over time rather than a snapshot in a lab report. Understanding how to identify early perimenopause hormonal shifts means looking at the trend of your symptoms over months, not days.

Cognitive & Emotional Changes: Brain Fog vs. Mood Swings
Perhaps the most distressing perimenopause symptoms are those that happen above the neck. Many women find themselves standing in a room forgetting why they walked in, or struggling to find common words during a meeting. When we look at perimenopause brain fog vs early onset dementia symptoms, it is important to understand the metabolic context. Estrogen plays a vital role in how the brain uses glucose for energy. As levels fluctuate, the brain undergoes a temporary energy crisis.
This neuro-metabolic shifts can lead to significant anxiety and mood swings. Estrogen influences the GABA and serotonin systems—the chemicals in your brain responsible for feeling calm and happy. When estrogen spikes and crashes, it can feel like your emotional "brakes" have been removed.
- Memory Lapses: Difficulty with word-retrieval or "tip-of-the-tongue" syndrome.
- Anxiety: Sudden feelings of panic or unease, even without a specific stressor.
- Sleep Fragmentation: Waking up at 3:00 AM due to the brain's reaction to dipping hormones.
Coping with anxiety and mood swings in early perimenopause often requires a dual approach: stabilizing the nervous system through lifestyle and, in some cases, hormonal support to level out the peaks and valleys. It is vital to remember that these cognitive shifts are usually a transition state. As the brain adapts to a lower-estrogen environment post-menopause, many women find their mental clarity returns.
Long-Term Health & Metabolic Insurance
While we often focus on the immediate perimenopause symptoms, this transition is also a critical window for "metabolic insurance." The hormonal shifts affect more than just your mood; they impact how you store fat and how your bones maintain their density. The average of four to seven years that this transition lasts is the ideal time to implement protective strategies.
One of the most common complaints is the shift in body composition, often referred to as perimenopause weight gain. As estrogen fluctuates, the body becomes more insulin resistant, and fat storage often shifts toward the abdomen. Lifestyle changes for perimenopause weight gain and metabolism should focus less on restrictive dieting and more on maintaining muscle mass. Resistance training becomes non-negotiable during this stage, as muscle helps maintain insulin sensitivity and supports cardiovascular health.

We must also look at bone health. The risk of osteopenia increases during the transition years. Supplementation with Vitamin K2 and Vitamin D is often recommended to ensure calcium is directed to the bones rather than the arteries. For some women, the benefits of regulated bioidentical hormone therapy for perimenopause (rBHRT) can be transformative, providing the steady floor of hormones needed to protect bone density and cardiovascular function while quieting the "chaos" of the transition.
Preparing for Your Consultation: Data-Driven Next Steps
Navigating the healthcare system during this transition can be frustrating. Many women are told they are "too young" for perimenopause or are offered antidepressants when their primary issue is hormonal. Preparing for perimenopause doctor visit with symptom tracking is your best tool for self-advocacy.
A 90-day symptom diary is the gold standard for clinical diagnosis. Instead of telling your doctor you "feel tired," you can show them that your cycles have shortened from 30 days to 23 days over the last six months, accompanied by night sweats on days 20 through 23. This data shifts the conversation from subjective feelings to objective clinical markers.
When preparing for perimenopause doctor visit, ask specifically about:
- The variability of your cycle and how it aligns with the STRAW+10 stages.
- Whether your symptoms warrant a trial of progesterone or bioidentical estrogen.
- Screening for cardiovascular health markers and bone density.
Remember, the goal of modern perimenopause management is not just to "survive" the symptoms, but to optimize your health for the decades that follow. You are the expert on your own body, and with the right data, you can ensure your transition is met with clinical precision and personal empathy.
FAQ
What are the first signs of perimenopause?
The earliest markers are usually changes in the menstrual cycle, such as cycles becoming shorter by several days, and the onset of sleep disturbances or night sweats. Emotional changes like increased irritability or a "wired" feeling before your period are also common early indicators.
How long does perimenopause usually last?
On average, the transition lasts between four and seven years. However, for some women, the phase can begin in the late 30s and persist for up to a decade before they officially reach menopause, which is defined as 12 consecutive months without a period.
How do I know if my symptoms are perimenopause or something else?
The best way to distinguish perimenopause from other conditions like thyroid dysfunction or stress is through longitudinal tracking. If your symptoms—such as brain fog, anxiety, or heavy bleeding—consistently follow a pattern related to your menstrual cycle, they are likely driven by hormonal shifts.
Does perimenopause cause anxiety and mood swings?
Yes, the volatility of estrogen significantly impacts brain chemistry, specifically affecting the GABA and serotonin receptors. This can lead to increased anxiety, sudden mood shifts, and a lower threshold for handling stress than you had in your younger years.
When should I see a doctor for perimenopause symptoms?
You should consult a healthcare provider if your symptoms are interfering with your quality of life, sleep, or work performance. Additionally, seek medical advice if you experience very heavy bleeding, periods that occur more often than every 21 days, or if you want to discuss long-term preventative health for your bones and heart.