Quick Facts
- Mechanism: GLP-1 medications regulate appetite by slowing down how quickly food leaves the stomach, a process known as gastric emptying.
- Risk Increase: Clinical research indicates that non-diabetic users of these drugs face a 3.67 times higher risk of developing gastroparesis compared to those on other weight loss medications.
- Incidence Rate: Real-world data shows an observed incidence rate of 0.53% among users, which translates to approximately 10 cases per 1,000 users for semaglutide.
- Primary Symptoms: Severe cases are marked by persistent nausea, frequent vomiting of undigested food hours after eating, and intense abdominal bloating.
- FDA Status: Updated FDA drug labels in 2026 now include specific warnings regarding the risk of severe delayed gastric emptying and potential stomach paralysis.
- Diagnosis: The gold standard for confirming GLP-1 gastroparesis is a 4-hour scintigraphy test to measure the precise rate of gastric motility.
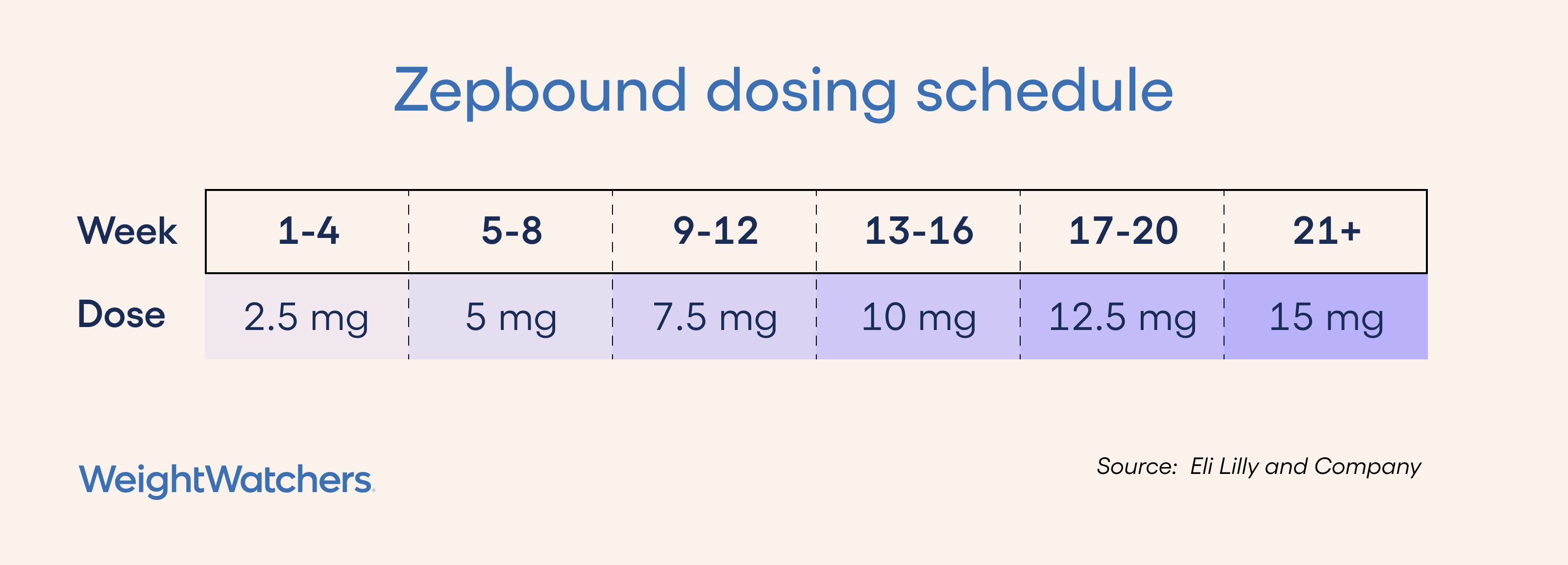
- Prevention: Medical experts recommend a start low, go slow titration strategy to allow the digestive system time to adapt to incretin mimetics.
GLP-1 medications like Semaglutide and Tirzepatide slow gastric motility to regulate appetite. However, in approximately 1-3% of users, this leads to clinical GLP-1 gastroparesis, a condition where stomach paralysis persists beyond the intended therapeutic effect.
The Mechanism: How GLP-1s Affect Gastric Motility
To understand why some people develop complications, we first have to look at how these medications function within the gut. Both Semaglutide and Tirzepatide are classified as incretin mimetics. They mimic natural hormones in the body that signal the pancreas to release insulin and the brain to feel full. A critical part of this satiety regulation happens in the gut wall, where these drugs bind to receptors that signal the stomach to slow down its contractions.
Under normal circumstances, this delay in gastric motility is helpful. It keeps food in the stomach longer, which helps stabilize blood sugar and prevents the quick return of hunger. However, for a small subset of patients, this slowing crosses the line from a therapeutic benefit into a clinical pathology. When the stomach muscles become too slow or stop moving entirely, we refer to it as stomach paralysis. Monitoring digestion while taking GLP-1 weight loss drugs is therefore not just about tracking weight, but about ensuring the biological transit of food remains functional.
The transition from healthy satiety to gastroparesis can be subtle. It often depends on the individual's baseline gut health, their dose, and how quickly they increased that dose. Because these drugs affect the autonomic nervous system’s control over the digestive tract, the biological "brakes" applied to the stomach can sometimes become stuck, leading to the severe symptoms reported in recent clinical trial data.
Normal Side Effects vs. Red Flags: When to Worry
It is common for patients to experience some level of nausea or changes in bowel habits when starting incretin mimetics. In fact, many clinical studies show that up to 40% of users experience mild gastrointestinal upset during the initial weeks of treatment. The challenge for the patient and the provider is recognizing early signs of GLP-1 gastroparesis before the condition leads to malnutrition or dehydration.
The following table helps distinguish between the expected adjustment period and the red flags that require immediate medical attention.
| Symptom | Normal Adjustment | Gastroparesis Red Flag |
|---|---|---|
| Nausea | Mild, usually occurs shortly after injection or a large meal. | Persistent, severe nausea that prevents any food intake. |
| Vomiting | Rare; usually triggered by overeating fatty foods. | Frequent vomiting of undigested food 6–12 hours after eating. |
| Fullness | Feeling satisfied with smaller portions. | Intense postprandial fullness after just a few bites; "brick in the stomach" feeling. |
| Pain | Occasional mild cramping or gas. | Severe, localized abdominal pain or cramping that does not resolve. |
| Weight Loss | Steady, intentional loss of 1–2 pounds per week. | Rapid, unintended weight loss due to the inability to keep food down. |
If you are wondering how to tell if GLP-1 nausea is actually gastroparesis, pay close attention to the timing of your symptoms. Standard side effects usually peak 24 to 48 hours after a dose and then taper off. In contrast, delayed gastric emptying symptoms tend to be persistent and may actually worsen as you attempt to eat normal meals. Chronic constipation can also be a secondary sign, as the slow movement in the stomach often reflects a slow-down throughout the entire intestinal tract.
Diagnosis: The 4-Hour Gastric Emptying Study
When a healthcare provider suspects that a patient’s delayed gastric emptying symptoms have reached a clinical level, they will typically order a specific diagnostic test. While blood work and physical exams provide clues, the definitive diagnosis of GLP-1 gastroparesis requires visualizing the stomach's transit time in real-time.
The Scintigraphy Test
The gold standard for diagnosis is the 4-hour gastric emptying study, which uses a technique called scintigraphy testing. During this procedure, the patient consumes a standardized meal—usually a small serving of egg whites or an egg substitute—that contains a tiny, safe amount of radioactive tracer.
Over the next four hours, a specialized camera takes images of the stomach at specific intervals (usually at 1, 2, and 4 hours). This allows technicians to calculate the exact percentage of food remaining in the stomach. Under normal conditions, more than 90% of the meal should have left the stomach by the 4-hour mark. If a significant amount of food remains, it confirms a diagnosis of stomach paralysis management needs.

Why the 4-Hour Window Matters
Shorter tests (such as 1-hour or 2-hour scans) are often inconclusive because many people have slightly slower digestion without it being pathological. The 4-hour mark is the clinical threshold used by gastroenterologists to ensure the diagnosis is accurate and not just a temporary fluctuation. This test also helps doctors determine if the issue is purely mechanical or if there are issues with nutrient absorption caused by the prolonged presence of food in the gastric chamber.
Management and Prevention Strategies
For those currently taking these medications or considering them, safety must be the priority. Most cases of GLP-1 gastroparesis can be managed if caught early, but prevention through careful medication use is always the better path.
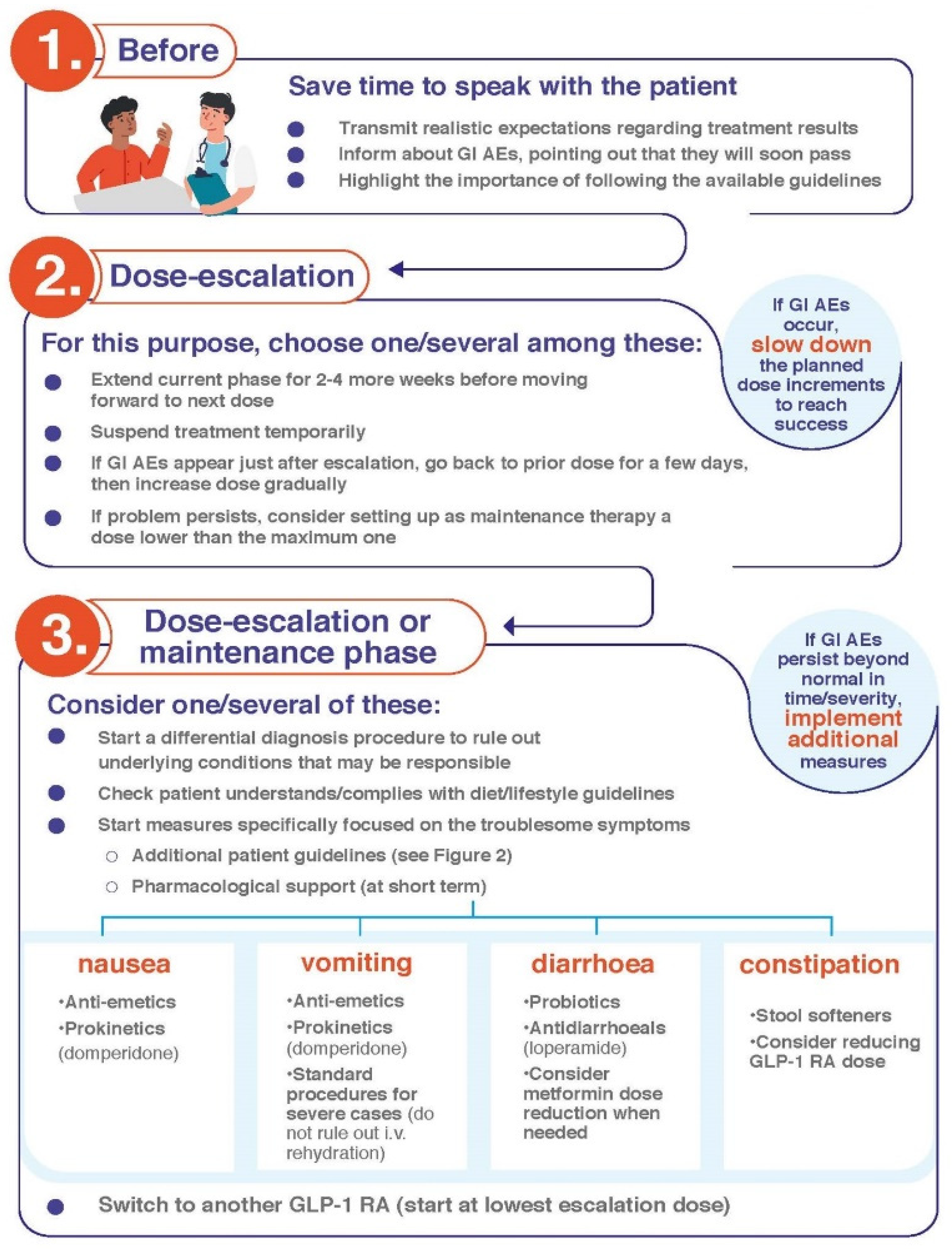
Titration and Monitoring
One of the most effective GLP-1 medication safety tips is the "start low, go slow" approach. Most manufacturers recommend a titration schedule that spans several months. Using safe GLP-1 titration strategies to avoid stomach paralysis involves staying at the lowest effective dose for as long as possible rather than rushing to the maximum dose. If you begin to feel significant fullness or nausea at a specific dose, it is a signal to pause the escalation and speak with your doctor.
Dietary Adjustments
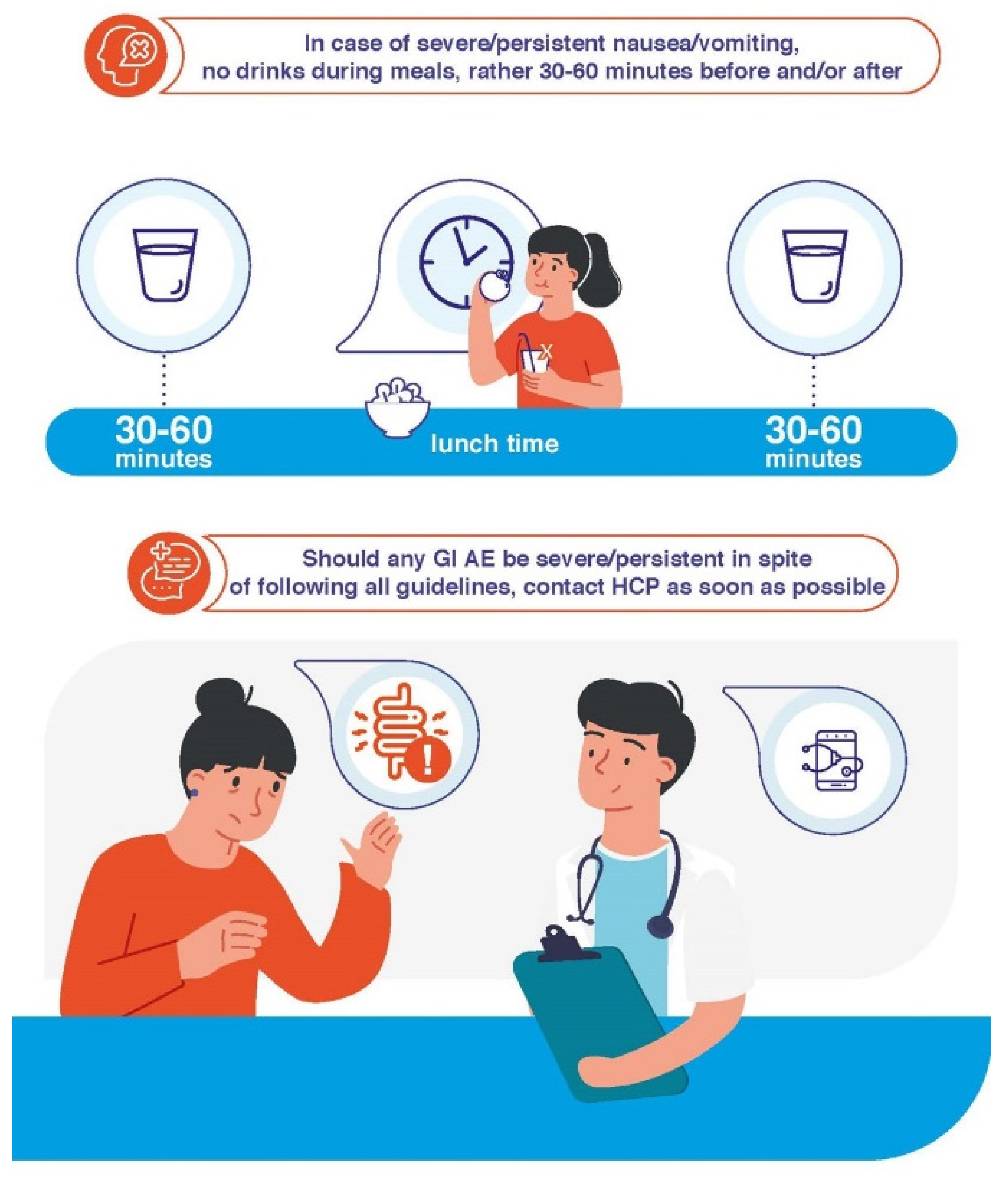
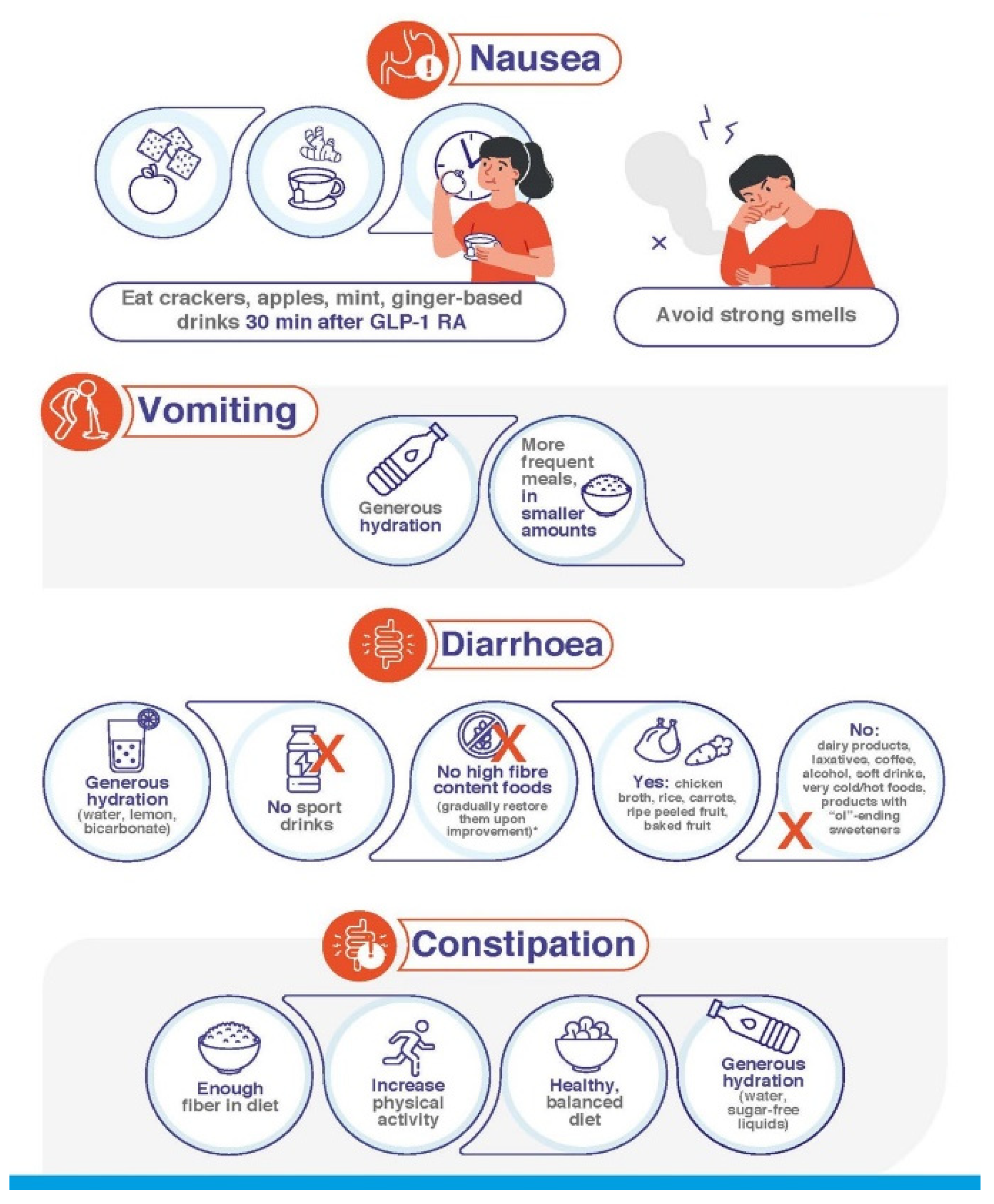
If you are managing GLP-1 induced delayed gastric emptying through diet, the goal is to reduce the workload on your stomach. This often involves:
- Eating smaller, more frequent meals (5–6 small snacks instead of 3 large meals).
- Choosing low-fiber and low-fat foods, as these are easier for the stomach to break down.
- Avoiding drinking through straws to reduce excess air in the stomach.
- Peeling all fruits and vegetables and cooking them until soft.
- Focusing on liquid nutrition if solid foods are not being tolerated well.
Many patients ask: is stomach paralysis from GLP-1 drugs reversible? In many documented cases, motility returns to normal once the medication is discontinued and has cleared the system. However, the clearance time for these drugs is long—often several weeks—so symptoms may persist for a month or more after the last injection.
2026 Safety Updates and Clinical Outlook
The landscape of GLP-1 therapy is changing rapidly as more long-term data becomes available. In 2026, the medical community saw significant updates to FDA drug labels for several major brands. These updates were driven by large-scale epidemiological studies that highlighted a higher incidence of gastrointestinal complications than initially reported in early clinical trial data.
A study published in the Journal of the American Medical Association (JAMA) found that patients using these agonists for weight loss had a 3.67 times higher risk of developing gastroparesis. Furthermore, research presented at the 2024 Digestive Disease Week conference indicated that users were 66% more likely to receive this diagnosis than non-users. While the absolute risk remains low—affecting less than 1% of the general user population—the risk increases significantly for those with pre-existing conditions like diabetic neuropathy, where the risk can be 3 to 5 times higher.

These updates serve as a reminder for both patients and clinicians to maintain open communication. If you are using these medications, ensure you are working with a provider who understands the nuances of gastric motility and who can help you navigate the balance between metabolic benefits and digestive health.
FAQ
Does GLP-1 cause permanent gastroparesis?
Current clinical evidence suggests that for most individuals, the delay in gastric emptying is a side effect of the medication's presence in the system. When the drug is discontinued, stomach motility typically returns to its baseline state over several weeks. However, because the half-life of these medications is long, recovery is not immediate. There is ongoing research into whether long-term use could cause permanent changes in very rare cases, particularly in those with underlying nerve damage.
What are the symptoms of stomach paralysis from GLP-1 drugs?
The hallmark symptoms include frequent vomiting of undigested food many hours after a meal, persistent and severe nausea, and a feeling of extreme fullness after consuming only a small amount of food. Other signs include significant abdominal bloating, upper abdominal pain, and unintended weight loss or malnutrition due to the inability to tolerate a normal diet.
How does GLP-1 medication affect stomach emptying?
These medications work as incretin mimetics, meaning they mimic hormones that naturally slow down the digestive process. They bind to receptors in the stomach and the nervous system to decrease the frequency and strength of stomach contractions. While this is intended to help with satiety and blood sugar control, it can sometimes slow the process so much that food remains in the stomach for an abnormally long time.
Can gastroparesis from GLP-1 agonists be reversed?
Yes, in the majority of reported clinical cases, the condition is reversible by stopping the medication. Since the drug causes a functional slowing rather than a structural blockage, removing the chemical signal that slows the stomach usually allows the muscles to resume their normal rhythm. Patients should work closely with their doctor to manage symptoms during the washout period, which can take 2 to 8 weeks.
How do doctors diagnose gastroparesis caused by GLP-1 medications?
Physicians typically begin with a physical exam and a review of symptoms, but the definitive diagnosis is made through a gastric emptying study. This involves eating a meal with a radioactive tracer and undergoing scintigraphy testing over a 4-hour period. If more than 10% of the food remains in the stomach after 4 hours, a diagnosis of gastroparesis is generally confirmed. Doctors may also use endoscopy to rule out physical obstructions in the digestive tract.