Quick Facts
- Intrinsic Rate: A standard junctional escape rhythm typically ranges between 40 and 60 beats per minute.
- Origin Point: The rhythm begins in the atrioventricular node or the Bundle of His rather than the sinoatrial node.
- ECG Markers: Key identifiers include a narrow QRS complex and P waves that are absent, inverted, or appear after the QRS.
- Nature: Primarily functions as a protective backup mechanism when the heart's natural pacemaker slows down or fails.
- Common Triggers: Triggers include high vagal tone, certain medications like beta-blockers, and conditions like sinoatrial node dysfunction.
- Clinical Outlook: Often benign in healthy individuals and athletes, but requires investigation if it causes symptoms like dizziness or fatigue.
A junctional rhythm occurs when the heart's electrical impulse originates from the atrioventricular (AV) node or the Bundle of His instead of the sinoatrial (SA) node. On an ECG, this typically presents with a regular rate of 40–60 beats per minute, narrow QRS complexes, and absent or inverted P waves. It often serves as a critical backup mechanism when the primary pacemaker fails, ensuring the heart continues to pump blood even when the main signal is interrupted.
What is Junctional Rhythm? The Heart's Backup System
To understand junctional rhythm, one must first visualize the heart's internal electrical grid. In a healthy heart, the sinoatrial node, located in the right atrium, acts as the primary pacemaker. It sends out regular electrical signals that coordinate the contraction of the heart muscle. This standard state is known as sinus rhythm. However, the heart is a remarkably resilient organ equipped with several fail-safes.
When the sinoatrial node fails to fire or the signal is blocked, the heart does not simply stop. Instead, secondary pacemakers take over. This is known as cardiac automaticity—the ability of different parts of the heart to spontaneously generate an electrical impulse. The most prominent backup is the atrioventricular node, situated at the junction between the atria and the ventricles. When the rhythm originates here, we call it a junctional rhythm.
Technically, a junctional rhythm is defined by a sequence of three or more consecutive beats originating from the AV junction. This serves as a physiological "safety net." If you compare junctional rhythm vs sinus rhythm, the primary difference lies in the starting point and the resulting speed. While sinus rhythm usually keeps the heart beating between 60 and 100 times per minute, the junctional rhythm is naturally slower, reflecting the intrinsic pace of the nodal tissue.
ECG Criteria: How to Identify Junctional Rhythm
For clinicians, the electrocardiogram (ECG) is the definitive tool for diagnosing this condition. Because the electrical signal starts in the middle of the heart rather than at the top, the "path" the electricity takes is altered. This change creates very specific visual markers on the ECG tracing.
When evaluating a strip for junctional rhythm ecg criteria, medical professionals look for the following checklist:
- Rate: Typically between 40 and 60 beats per minute for an escape rhythm.
- Rhythm: Usually very regular.
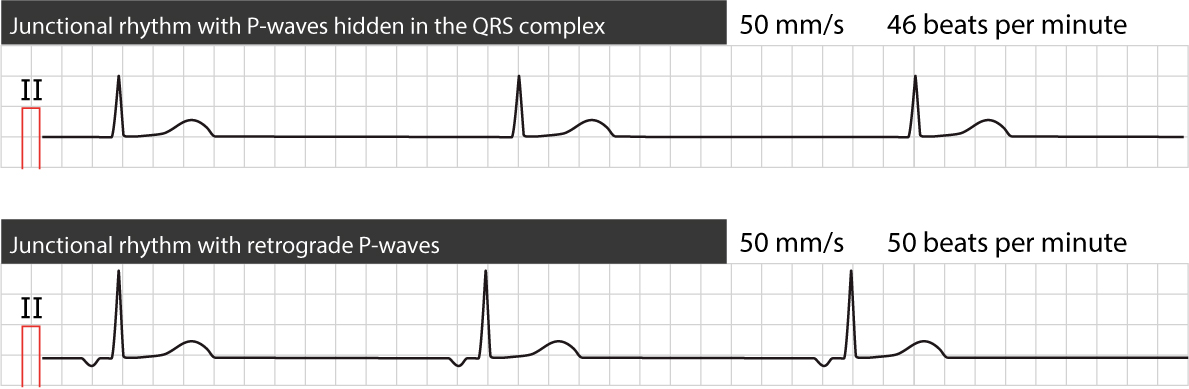
- P Waves: These are often the most telling sign. Because the signal may travel backward toward the atria (retrograde conduction), the P waves might be inverted (upside down), hidden within the QRS complex, or appear immediately after the QRS complex.
- PR Interval: If a P wave is visible before the QRS, the PR interval is usually very short (less than 0.12 seconds).
- QRS Complex: Because the signal travels down the normal pathways into the ventricles, the narrow QRS complex remains intact, usually measuring less than 0.12 seconds.
The presence of inverted P waves is a hallmark of the signal's origin. In a normal sinus beat, the electricity flows downward, creating an upright P wave. In a junctional beat, the electricity must travel "upstream" to reach the atria, which flips the wave on the graph. If the signal reaches the atria and ventricles at the exact same time, the larger electrical force of the ventricles completely hides the P wave, making it appear absent.

The Four Types of Junctional Rhythms
Not all junctional rhythms are created equal. They are categorized primarily by the speed at which the junction is firing. While the intrinsic rate for a junctional escape rhythm typically ranges from 40 to 60 beats per minute, which serves as a physiological backup when the primary sinoatrial node fails, other variations exist.
| Rhythm Type | Heart Rate (BPM) | Clinical Context |
|---|---|---|
| Junctional Bradycardia | Less than 40 bpm | Often pathological; may require intervention if the patient is symptomatic. |
| Junctional Escape Rhythm | 40 – 60 bpm | The most common "backup" form; often seen in healthy people during sleep. |
| Accelerated Junctional Rhythm | 60 – 100 bpm | Not technically a tachycardia, but faster than the junction's natural rate. |
| Junctional Tachycardia | Greater than 100 bpm | A rapid rhythm that can cause hemodynamic instability. |
An accelerated junctional rhythm is defined by a heart rate between 60 and 100 beats per minute, whereas junctional tachycardia is diagnosed when the rate exceeds 100 beats per minute. These faster rhythms are often caused by increased irritability of the AV node tissue. One specific and serious form is postoperative junctional ectopic tachycardia, which occurs in approximately 5% to 11% of pediatric patients who undergo surgery to correct congenital heart defects.
In adults, management of accelerated junctional rhythm often involves looking for underlying irritation, such as inflammation or toxicity. Ensuring hemodynamic stability is the priority, meaning the doctor will check if the heart is still pumping enough blood to maintain blood pressure and oxygenate the brain.
Is it Normal? Benign vs. Pathological Causes
One of the most common questions patients ask is: "Is this heart rate normal?" The answer depends entirely on the context. For some, a junctional rhythm is a sign of an elite cardiovascular system; for others, it is a warning sign of underlying illness.
Benign Causes: The Athletic Heart
In well-trained athletes, the heart is often so efficient that the resting sinus rate drops significantly. This is due to high Vagal tone, a state where the nervous system slows the heart to conserve energy. If the sinus rate drops below 40 bpm, the AV node may take over. This is why is junctional rhythm normal in athletes is a frequent topic in sports medicine. It is also common to see this rhythm in healthy young people during deep sleep, as it represents a normal physiological transition.
Pathological Junctional Rhythm Causes
When the rhythm appears during normal daily activity in a non-athlete, doctors look for junctional rhythm causes that might indicate a problem. These include:
- Sinoatrial node dysfunction: Also known as sick sinus syndrome, where the primary pacemaker simply wears out or becomes damaged.
- Myocardial ischemia: Reduced blood flow to the heart muscle, often during a heart attack, can damage the electrical pathways.
- Electrolyte imbalance: Abnormal levels of potassium, calcium, or magnesium can interfere with the electrical signals.
Medication Warning: Several common drugs can suppress the SA node or speed up the AV junction. Digoxin toxicity is a classic cause of accelerated junctional rhythms. Additionally, medications that cause junctional rhythm include beta-blockers and calcium channel blockers, which are often prescribed for high blood pressure or anxiety.
Symptoms and When to See a Doctor
Because a junctional rhythm is usually slower than a sinus rhythm, it may not always meet the body's demand for oxygenated blood. Many people with a junctional escape rhythm are completely asymptomatic and only discover the condition during a routine physical or an ECG for an unrelated issue.
However, when the rate is too slow to maintain cardiac output, several junctional rhythm symptoms may emerge:
- Dizziness or lightheadedness
- Unusual fatigue or lethargy
- Shortness of breath, especially during exertion
- Syncope (fainting)
- A sensation of skipped beats or "heart pounding"
- Low blood pressure (hypotension)
Knowing when to seek medical help for junctional rhythm is vital. If you experience sudden fainting, chest pain, or severe shortness of breath, you should seek emergency care immediately. If your heart rate is consistently below 50 beats per minute and you feel "off" or chronically tired, a consultation with a cardiologist is recommended.
Diagnostic management focuses on identifying the underlying etiology. This may involve blood tests to check for electrolyte imbalance, a stress test, or an electrophysiology study to map the heart's signals. In cases where the rhythm is caused by medications, adjusting the dosage often resolves the issue. If the cause is permanent SA node failure, a pacemaker may be necessary to restore a healthy heart rate.
FAQ
What is junctional rhythm?
Junctional rhythm is a heart rhythm that originates from the atrioventricular node or the Bundle of His. It serves as a backup electrical signal when the heart's primary pacemaker, the sinoatrial node, is either too slow or failing to send signals. It is characterized by a heart rate typically between 40 and 60 beats per minute.
Is a junctional rhythm dangerous?
By itself, a junctional rhythm is not necessarily dangerous; it is often a life-saving backup mechanism. However, its danger depends on the heart rate and the cause. If the rate is too slow to support the body's needs (causing low blood pressure) or if it is a symptom of heart damage or drug toxicity, it requires medical attention.
What are the common causes of junctional rhythm?
Common causes include high vagal tone (common in athletes and during sleep), sinoatrial node dysfunction, and certain medications like beta-blockers or digoxin. Other causes include heart surgery, electrolyte imbalances, and myocardial ischemia or heart attacks that affect the heart's electrical system.
What are the symptoms of junctional rhythm?
Many people have no symptoms. Those who do may experience dizziness, fatigue, fainting spells, shortness of breath, or a general feeling of weakness. These symptoms occur because the slower heart rate may not pump enough blood to the rest of the body.
How is junctional rhythm diagnosed?
The primary method of diagnosis is an electrocardiogram (ECG). A doctor looks for specific patterns, such as a heart rate of 40-60 beats per minute, a narrow QRS complex, and P waves that are either missing, upside down (inverted), or occurring after the main heartbeat signal.
While discovering an "abnormal" heart rhythm can be unsettling, a junctional rhythm is often just a sign that your heart's built-in safety features are working exactly as intended. Whether it is the result of an athletic lifestyle or an underlying medical condition, the key is professional evaluation. If you have noticed changes in your heart rate or are experiencing new symptoms like dizziness, speaking with a healthcare provider can provide both clarity and a plan for long-term heart health.